Lethal Injection: The Myth of Painless Death
Lethal injection was designed in 1977 by someone who admitted he had no idea if it would work. A 2005 Lancet study found 43% of prisoners may have been conscious during execution.
Lethal Injection: The Myth of Painless Death
Lethal injection was sold as a medical solution to a political problem. By the 1970s, the electric chair and the gas chamber had accumulated enough documented botches — flames, coughing, apparent suffering — that capital punishment’s supporters needed something that looked cleaner. Oklahoma legislated lethal injection in 1977 based on a protocol designed by two people with no pharmacological expertise: a medical examiner named Jay Chapman and a state senator named Bill Dawson. Chapman later admitted he had “no idea” if the three-drug protocol he designed would work as intended. It became the standard method for executions across the United States, and it has been producing botched executions ever since.
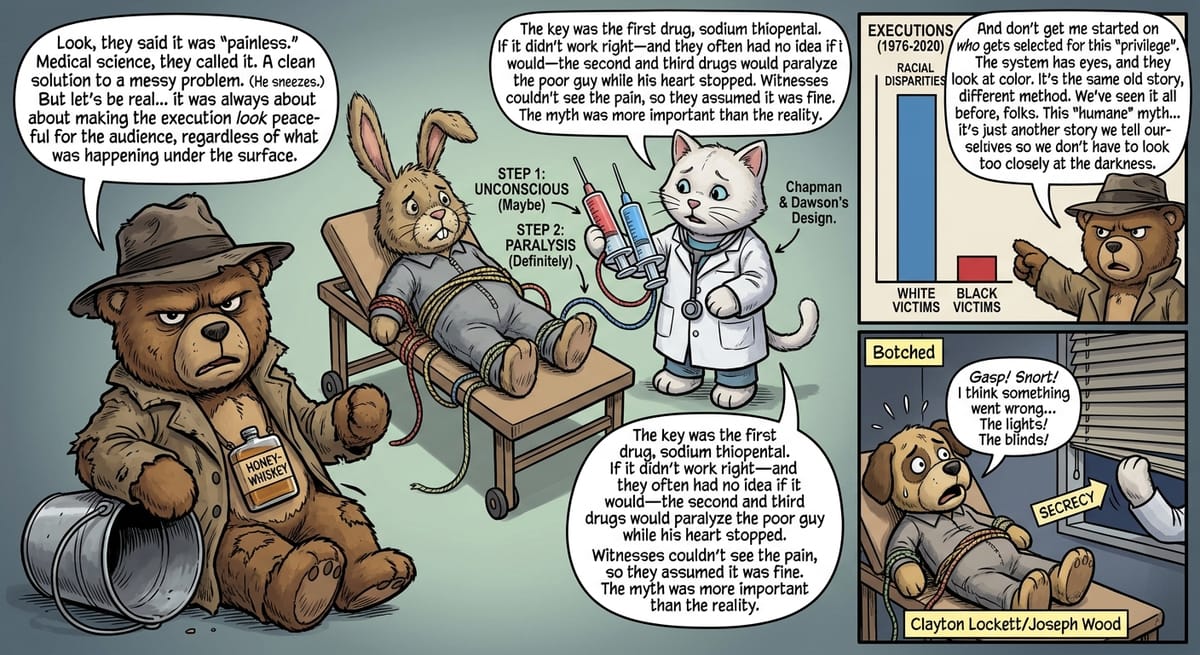
The Three-Drug Protocol Was Designed to Look Peaceful, Not to Be Peaceful
The three-drug protocol Chapman designed — and which most states adopted with minimal modification — works in three steps. First, sodium thiopental, a barbiturate, is administered to induce unconsciousness. Second, pancuronium bromide, a paralytic agent, stops the prisoner’s breathing. Third, potassium chloride stops the heart. The sequence is designed so that the prisoner is unconscious before the second and third drugs are administered, because the paralytic causes suffocation and the potassium chloride causes intense pain as it disrupts cardiac function.
The problem is the first drug. If sodium thiopental is administered in insufficient quantity, or if the prisoner has a higher tolerance than expected, or if the IV is improperly placed, the prisoner may remain conscious during the administration of the second and third drugs — paralyzed and unable to show distress while experiencing what witnesses would recognize as suffering if they could see it. The paralytic drug ensures that an inadequately sedated prisoner appears calm to observers. The protocol was designed, in other words, to produce a peaceful-looking death regardless of what the prisoner actually experiences.^1^
The Lancet published a study in 2005 by researchers at the University of Miami who reviewed toxicology reports from 49 executed prisoners in four states and found that 43 percent had blood levels of anesthetic suggesting possible awareness during execution. The authors concluded that lethal injection “may mask the signs of pain and suffering.” The study did not prove that those prisoners suffered, but it established that the protocol provided no guarantee they had not.
What Happened When States Ran Out of the Drug?
The United States has always imported sodium thiopental, used in lethal injection, from European manufacturers. In 2011, the European Union moved to restrict exports of drugs used for execution — a response to years of advocacy by European human rights organizations. The drug’s sole U.S. manufacturer had already discontinued production. States suddenly found themselves unable to obtain the drug their protocols required.
The improvisation that followed revealed the gap between lethal injection’s medical pretensions and its actual execution. States experimented with replacement drugs and replacement protocols. Ohio switched to a single-drug protocol using midazolam, a sedative, in 2014. Arizona used midazolam in the execution of Joseph Wood on July 23, 2014; Wood took nearly two hours to die, gasping and snorting throughout the process in a way witnesses found clearly inconsistent with unconsciousness. The state’s corrections director described the execution as “textbook.” Witnesses disagreed.^2^
Oklahoma used midazolam in the execution of Clayton Lockett on April 29, 2014. The IV was improperly placed and the drug did not fully enter Lockett’s bloodstream. Lockett regained consciousness during the execution, tried to speak, and was observed writhing on the gurney before dying of a heart attack 43 minutes after the procedure began. The execution chamber’s blinds were lowered to prevent witnesses from observing the conclusion. Oklahoma’s subsequent investigation found that officials had proceeded despite warning signs about the IV and the drug protocol.^3^
Racial Disparities in Who Gets Executed Define the Practice
The population of people executed by lethal injection in the United States reflects the same racial and economic disparities as the broader criminal justice system. A 2020 study by the Death Penalty Information Center found that since 1976, when the Supreme Court reinstated capital punishment in Gregg v. Georgia, 76 percent of executions have involved cases where the victim was white, despite the fact that homicides in the United States are roughly equally divided between white and non-white victims. Black defendants convicted of killing white victims are significantly more likely to receive death sentences than white defendants convicted of killing Black victims.^4^
The people who are executed are also disproportionately those who could not afford effective legal representation. The Supreme Court’s 2002 decision in Atkins v. Virginia prohibited the execution of people with intellectual disabilities, and its 2005 decision in Roper v. Simmons prohibited the execution of people who were under 18 at the time of their crime. The execution of people with serious mental illness remains legal. Several men on death row have been diagnosed with schizophrenia; their executions have proceeded when courts have found them competent to understand what was happening to them.
The Medical Appearance Is the Point, and the Secrecy Protects It
The American Medical Association, the American Board of Anesthesiology, and other medical professional organizations have issued guidelines prohibiting physician participation in executions. The AMA’s position, adopted in 1980 and reaffirmed multiple times, is that physician participation in capital punishment is a fundamental violation of the healing relationship. This has created an ongoing problem for states attempting to conduct lethal injections that approximate medical procedure: the people with the most relevant expertise are professionally prohibited from participating.
States have responded by using medical professionals with lesser training, prison personnel, or anonymous individuals. The identities of the people who administer lethal injections are routinely shielded by state secrecy laws, making it impossible to verify the qualifications of the people conducting what is presented to the public as a medical procedure. The gap between the medical appearance of lethal injection and its actual execution is a feature, not a bug — the medical framing is what makes the practice politically sustainable, and the secrecy is what prevents scrutiny of whether it lives up to that framing.
Lethal injection continues as the dominant method in every state that practices capital punishment, despite a decades-long accumulation of evidence that the protocols do not reliably produce the painless death they are advertised to produce. The myth of humane killing, which drove the electric chair’s invention and the gas chamber’s adoption before it, has driven lethal injection since 1977. It has never been dispelled — only periodically, and embarrassingly, tested.
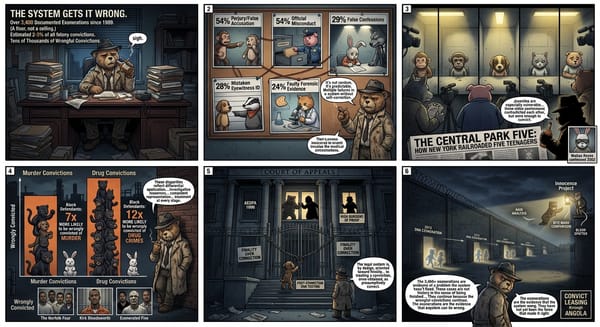
The Innocence Project has documented 21 people exonerated from death row after DNA testing proved their innocence — people who came within the reach of this protocol based on convictions that turned out to be wrong. The Central Park Five case is one illustration of how those wrongful convictions happen.
─────────
Sources:
- Denno, Deborah W. “The Lethal Injection Quandary: How Medicine Has Dismantled the Death Penalty.” Fordham Law Review 76, no. 1 (2007).
- Stern, Mark Joseph. “Arizona’s Horrific Execution: The Latest Lethal Injection Debacle.” Slate, July 23, 2014.
- Oklahoma Department of Public Safety. Investigation Into the Execution of Clayton D. Lockett. November 2014.
- Death Penalty Information Center. Racial Disparities in U.S. Executions, 1976–2020. 2020.
Part of A History of Punishment — ← Back to series hub