Meth in Rural America: The Drug That Ate Small Towns
Methamphetamine grew from within rural America in the 1990s — out of farm communities watching their economies collapse. Twelve thousand meth labs seized in 2001 alone before Mexican cartels took over the market.
Meth in Rural America: The Drug That Ate Small Towns
The methamphetamine epidemic arrived in rural America differently than crack arrived in cities — it grew from within, out of the same farm communities and trailer parks that had been watching their economies collapse since the 1980s. For much of the 1990s and into the early 2000s, meth in rural America was made where it was used, by people who were also using it, with precursor chemicals available at any farm supply store.^1^ The consequences — addiction, burns, toxic contamination, family dissolution — were intimate and local in a way that made them harder to see and slower to address than the urban crack epidemic had been.
Part of Meth and the Opioid Crisis — ← Back to series hub
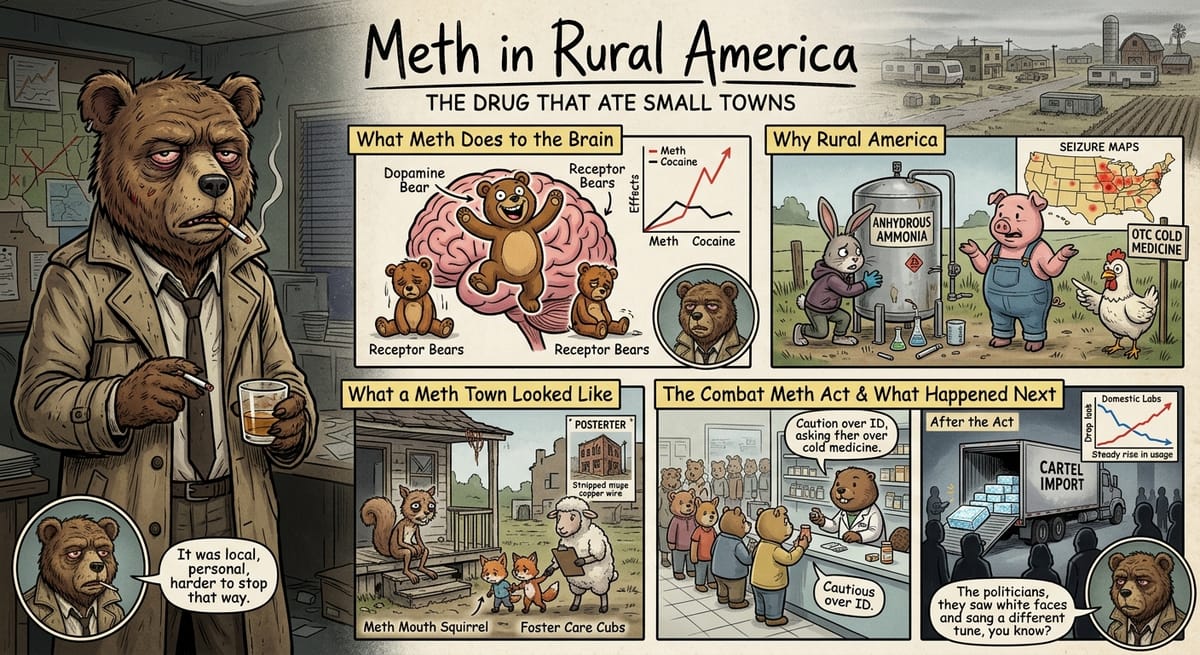
What Methamphetamine Does to the Brain
Methamphetamine is a synthetic stimulant that acts on the central nervous system by causing the release of large amounts of dopamine, norepinephrine, and serotonin — a surge that produces intense euphoria, increased energy and alertness, and suppressed appetite. Unlike cocaine, which clears the brain relatively quickly, methamphetamine effects can last 8 to 12 hours, with dopamine levels in the brain rising approximately three times higher than cocaine produces.
The neurological damage from chronic meth use is well-documented. It degrades dopamine receptors and dopamine transporters, effectively reducing the brain’s capacity to experience pleasure through normal means. Studies published by the Proceedings of the National Academy of Sciences in 2001, by Dr. Nora Volkow and colleagues at Brookhaven National Laboratory, showed partial recovery of dopamine function after 14 months of abstinence, with some deficits persisting for years.^2^
Why Rural America Was Where Meth Took Root
The meth epidemic’s geographic concentration in rural areas was not accidental. Methamphetamine can be synthesized from pseudoephedrine — a decongestant available in over-the-counter cold medicines — combined with common chemicals including acetone, anhydrous ammonia (used as fertilizer), and red phosphorus. The anhydrous ammonia connection was particularly significant in the rural Midwest and Plains: it was available on farms, often in unlocked storage tanks, and its theft became a significant agricultural crime problem throughout the 1990s.
The Drug Enforcement Administration began systematically tracking methamphetamine lab seizures in the 1990s. In fiscal year 2001, the DEA recorded 12,715 lab seizures nationally, with the highest concentrations in Missouri, California, Iowa, Indiana, and Oklahoma. Missouri alone accounted for more than 2,000 seizures in some years.^3^
The labs were dangerous beyond their product. The synthesis process generates approximately six pounds of toxic chemical waste for every pound of methamphetamine produced and creates explosion and fire risks. From 1999 to 2004, more than 1,500 meth lab fires or explosions were recorded nationally. Children who were present in homes where meth was being produced were exposed to toxic chemicals and removed to foster care at rates that overwhelmed rural child welfare systems — Iowa saw its meth-related child removals increase more than 100 percent between 2000 and 2003.
What a Meth Town Actually Looked Like
The sociological footprint of rural meth in the late 1990s and early 2000s is documented most comprehensively in journalism and public health research from the counties most affected. Nick Reding’s 2009 book Methland, which followed the town of Oelwein, Iowa (population approximately 6,000), through its meth epidemic, is the most thorough single account. Oelwein had lost its primary employer — a meatpacking plant — in the 1980s, and economic dislocation had produced the conditions that made meth attractive. The drug offered energy for second and third shift workers, weight loss in a culture that valued thin women’s bodies, and an intensity of experience that a shrinking economy and shrinking social world could not provide.
The physical toll was visible in ways that statistics cannot fully capture: dental decay (“meth mouth”) visible in people in their thirties who looked decades older, children in foster care in numbers that small-town systems were not built to handle, property crimes rising as people stripped copper from buildings and stole anhydrous ammonia from farm tanks to fund or supply the habit.^1^
What Congress Did to Stop It — and What Happened Next
Congress’s primary supply-side response was the Combat Methamphetamine Epidemic Act of 2005, signed by President George W. Bush on March 9, 2006. The law placed pseudoephedrine behind the pharmacy counter, requiring purchasers to show identification and limiting purchase quantities. It created a national tracking system that allowed pharmacies to flag attempts to purchase above the legal threshold.
The law was effective in reducing domestic meth lab production. Lab seizures dropped from the 12,000-plus annual peak to approximately 5,000 by 2010 and continued declining. But the drug did not become less available. Mexican drug trafficking organizations — the Sinaloa Cartel and others — filled the supply gap with high-purity methamphetamine produced in industrial labs in Mexico and transported across the border. The product they distributed was often purer and cheaper than what domestic labs had produced, and it reached rural markets through the same distribution networks that had moved it before. Reducing domestic production had shifted the supply chain without reducing the demand.^3^
Why the Political Response to Meth Was Different From Crack
The demographics of methamphetamine use in rural America were significantly different from the demographics of urban crack use. Meth’s rural user base was predominantly white, spread across age ranges that included working adults, not just young men, and included substantial numbers of women. The National Survey on Drug Use and Health data from the mid-2000s showed that methamphetamine use was roughly equally distributed by gender in rural areas — a pattern distinct from crack, which was more heavily male.
This demographic difference had a real effect on the political response. The meth epidemic in rural white communities generated a more explicitly public health-oriented response from politicians and law enforcement than the crack epidemic had in Black urban communities — more conversation about treatment resources, more acknowledgment of addiction as a disease, more sympathy for the communities affected. Whether this difference was driven by race, by geography, or by the accumulation of evidence about the failure of enforcement-first approaches, it was visible and consistent.
The rural meth epidemic peaked in the early-to-mid 2000s and declined significantly after the Combat Methamphetamine Epidemic Act reduced domestic production. But it did not disappear — it transformed. Mexican supply chains replaced domestic labs, producing a meth market that was, if anything, more consistent and better-supplied than what the lab era had provided. By the mid-2010s, meth overdose deaths were increasing again, driven now by Mexican product flooding rural and suburban markets. The drug that had eaten small towns in the 1990s came back in a different form, more potent, cheaper, and this time without even the local production infrastructure that had given some communities a visible target to combat. The opioid crisis followed a similar arc: enforcement closed one door, and the market walked through another.
─────────
Sources:
- Reding, Nick. Methland: The Death and Life of an American Small Town. Bloomsbury, 2009.
- Volkow, Nora D., et al. “Loss of Dopamine Transporters in Methamphetamine Abusers.” Proceedings of the National Academy of Sciences, 2001.
- Drug Enforcement Administration. National Methamphetamine Threat Assessment. U.S. Department of Justice, 2006.
- Weisheit, Ralph and William White. Methamphetamine: Its History, Pharmacology, and Treatment. Hazelden, 2009.
- Sexton, Rocky L., et al. “Methamphetamine Use Among Rural and Small-Town Adults in the United States.” Substance Use & Misuse, 2006.